Bereavement during the Covid-19 pandemic in the UK: What do we know so far?
Emily Harrop
Cardiff University, Marie Curie Palliative Care Research Centre, Division of Population Medicine
Lucy E Selman
University of Bristol, Palliative and End of Life Care Research Group, Population Health Sciences, Bristol Medical School
Abstract
The
Covid-19 pandemic has been a devastating mass bereavement event, with measures
to control the virus leading to unprecedented changes to end-of-life and
mourning practices. In this review we consider the research evidence on the
experiences of people bereaved during the pandemic. We summarise
key findings reported in the first five publications from our UK-based Bereavement during COVID-19 study,
drawing comparisons with available evidence from other studies of bereavement
during the pandemic. We summarise these findings
across three main topics: experiences at the end of life and in early
bereavement; coping and informal support during the pandemic; and access to
bereavement and mental health services. The synthesis demonstrates the
exceptional challenges of pandemic bereavement, including high levels of
disruption to end-of-life care, dying and mourning practices as well as to
people's social networks and usual coping mechanisms. We identified
considerable needs for emotional, therapeutic and informal support among
bereaved people, compounded by significant difficulties in receiving and
accessing such support. We provide evidence-based recommendations for improving
people's experiences of bereavement and access to support at all levels.
Practice points
1. Improve communication with families at the end of life, enabling visiting and contact with patients as far as possible and providing better support immediately after a death. This post-death contact should include information-giving on bereavement services and opportunities to discuss the death/patient-care.
2. Greater resourcing and expansion of national and regional adult and child bereavement services, with strategies to improve awareness of bereavement support options for adults and children and young people. Information on services and self-help resources should be widely available in online and community settings.
3. Community, school and work-based based interventions/guidance should strengthen supportive networks and improve grief literacy, compassion and communication skills across society. When lockdown restrictions are in place, more flexible support bubbles should be permitted for the recently bereaved.
4.
Provide opportunities for remembrance,
greater respect and listening to those bereaved, including national and local
initiatives which support private and public remembrance; and inclusive
consultation with those recently bereaved (eg via the
UK Commission on Bereavement: bereavementcommission.org.uk)
Keywords
bereavement, grief, pandemics, coronavirus infections, bereavement services
As we
approach the second anniversary of the first Covid-19 reported deaths in the
UK, we consider the growing body of research evidence on the experiences of
people bereaved during this most devastating and disruptive of global
pandemics. We summarise key findings reported in the
first five publications from our UK-based Bereavement
during Covid-19 study, drawing comparisons with available evidence from
other studies investigating the experiences of bereaved people during Covid-19.
The Bereavement during COVID-19 study
includes a mixed-methods longitudinal survey investigating end-of-life
experiences (including experiences of care before and immediately after the
death), bereavement support needs and experiences in the UK during Covid-19.
Baseline data was collected from people bereaved in the UK from 16 March 2020
(of any cause of death), when the first infection control restrictions were
implemented, until 2 January 2021. The survey was open from 28 August 2020 to 5
January 2021 and was completed by 711 adults who had been bereaved between 1
and 279 days ago (median 152 days (5 months)).
The study
publications summarised here report on interim (Harrop et al, 2020) and full results from the baseline
survey (Harrop et al, 2021a; 2021b; Selman et al,
2021a; Torrens-Burton et al, 2021). We also include in the summary a
publication reporting results from the second round survey responses of 104
parent/guardian participants, who answered a question on the support
experiences and needs of their children, aged 25 or under (Harrop
et al, 2021b).
Here we summarise study findings to date in three main topics:
experiences at the end of life and in early bereavement; coping and informal
support during the pandemic; and access to bereavement and mental health
services.
Sample characteristics
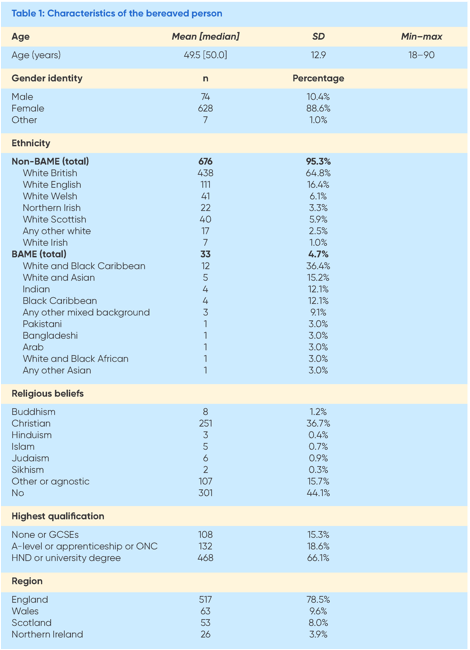
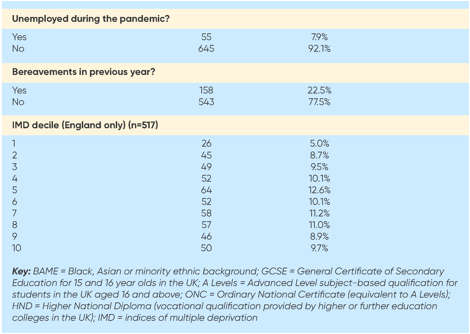
Participant
characteristics are presented in Table 1. Participants represented diverse
geographical areas, deprivation indexes and levels of education. 88.6% of
participants were female (n=628); the mean age of the bereaved person was 49.5
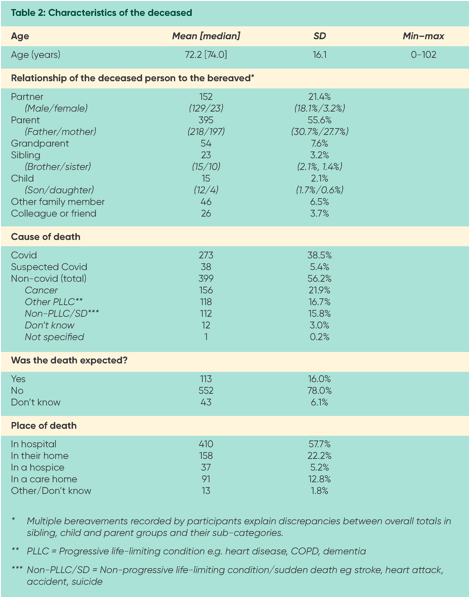
years old (SD = 12.9; range 18-90). The most common relationship of the
deceased to the bereaved was parent (n=395,55.6%), followed by partner/spouse
(n=152,21.4%). 72 people (10.1%) had experienced more than one bereavement
since 16 March 2020. 33 people (4.7%) self-identified as from a minority ethnic
background. The mean age of the deceased person was 72.2 years old (SD=16.1;
range during pregnancy to 102 years) (Table 2). 43.8% (n=311) died of
confirmed/ suspected Covid-19, 21.9% (n=156) from cancer, and 16.7% (n=119)
from another life-limiting condition. Most died in hospital (n=410; 57.8%).
Experiences at the end of
life and in early bereavement
We found
almost all participants were affected by the restrictions placed on family
visiting in health and care settings, funerals and everyday social interaction.
These included restricted funerals (93%), limited contact with other close
relatives or friends (80%), loneliness and social isolation (67%) and being 'unable
to say goodbye as I would have liked' (64%). There was wide variation in
overall reported experiences of end-of-life care; for example, while 21.8%
reported they were always involved in decision about the care of their loved
one, 21.8% reported that they were never involved; 32.3% reported that they
were fully informed about the approaching death while 17.7% said they were not
at all informed (Selman et al, 2021a). Lack of support following the death was
a major issue, with 35.4% of participants reporting that they felt 'not at all'
supported by professionals immediately after the death. Similar problems have
been reported in pandemic bereavement studies conducted in the Netherlands, UK
and USA (Becque et al, 2021; Hanna et al, 2021; Mayland et al; 2021; Neimeyer
& Lee, 2021). Problems communicating with healthcare providers (HPCs)
related to difficulty getting information about their family member, being
misinformed about their condition and hospital policies and not being involved
in care or treatment decisions (Harrop et al, 2020;
Torrens-Burton et al, 2021). More positive experiences included being treated
with compassion and kindness, being able to visit, and relatives feeling that
they were kept well-informed about their family member's condition and care (Harrop et al, 2020). Again, these findings are consistent
with results from Dutch and UK studies (Becque et al,
2021; Hanna et al, 2021; Mayland et al, 2021).
We identified
several risk factors for problematic experiences towards the end of life and in
early bereavement including place of death and whether the death was expected
or not (Selman et al, 2021a). Deaths in hospital/care home compared with in
hospice/at home increased the likelihood of the bereaved person being unable to
visit prior to death or say goodbye as they wanted. By
contrast, deaths that occurred in hospice/at home, and deaths that were
expected increased the likelihood of the bereaved person being involved in care
decisions and feeling well supported by healthcare professionals after the
death. Bereavement due to Covid-19, compared with all other types of deaths,
decreased the likelihood of being involved in care decisions and of feeling
well supported by HCPs after the death, while increasing the likelihood of
being unable to say goodbye (Selman et al, 2021a).
Our
qualitative results demonstrate the emotional and psychological impacts of
these experiences (Torrens-Burton et al, 2021). People described the distress
and guilt caused by being unable to say goodbye and provide comfort to their
dying relative, as observed in the other UK study (Hanna et al, 2021; Mayland et al, 2021). Parents also described the added
confusion and upset caused to their children by being separated from
grandparents before the death (Harrop et al,
2021b). Having unanswered questions, regrets and doubts made it harder to
process and reconcile their feelings surrounding the death (Torrens-Burton et
al, 2021). Reflecting these difficulties, 60% of participants reported
experiencing high or fairly high needs for help 'dealing with my feelings about
the way my loved one died' (Harrop et al, 2021a).
Restricted funeral and memorialisation practices,
inability to support one another and mourn collectively also made it difficult
to find closure and begin to grieve (Torrens-Burton et al, 2021). These grief
difficulties are consistent with the quantitative findings of a US pandemic study, that 'disrupted meaning' contributed to worse grief
outcomes, and that higher levels of functional impairment occurred for
all deaths during Covid19 compared with pre-pandemic times (Menzies
et al, 2020; Breen et al, 2021).
Coping and informal
support during the pandemic
Participants
described the overwhelming and dehumanising effect of
being bereaved at a time of mass bereavement, with one in ten experiencing
multiple deaths. This was exacerbated by insensitive and
prolonged reporting of death statistics and other negative media coverage
(Torrens-Burton et al, 2021), observed also in analyses of UK media coverage
during the pandemic (Selman et al, 2021b; Sowden
et al, 2021). People found it harder to openly grieve, and experienced anger
and alienation in response to perceived government incompetence, conspiracy
theories questioning the pandemic, and public disregard of social-distancing
requirements and regulations (Torrens-Burton et al, 2021). Similar observations
were reported in an analysis of Twitter data from bereaved family members and
friends (Selman et al, 2021c) and another UK survey of bereaved people
conducted early in the pandemic (Sue Ryder, 2020). Adding to this upset, many
people described the further stress and distress that they encountered as they
tried to organise the affairs of their deceased
relative, particularly amidst the organisational
chaos of lockdown (Torrens-Burton et al, 2021). Around a quarter of
participants reported high/fairly high needs for help with administrative tasks
and accessing financial and legal information and advice (Harrop
et al, 2021a).
When
lockdown restrictions were in place, people struggled with not being able to
visit friends, engage in social and recreational activities and experience
respite from their situation. Fear of catching or spreading Covid-19 also
affected people's ability to cope and go about their daily lives, particularly
among those bereaved by the virus (Torrens-Burton et al, 2021). Consistent with
these challenges, around a half of people reported high/fairly high needs for
help with 'loneliness and isolation', 'feeling comforted and reassured', 'finding
balance between grieving and other areas of life' and 'regaining sense of
purpose and meaning in life' (Harrop et al, 2021a).
Social isolation and loneliness were also found to be especially prevalent
among people bereaved by a Covid-19 death and among bereaved partners (Selman
et al, 2021a). This contrasts with results from one of
the Netherland surveys, which found that satisfaction with social support did
not differ between people bereaved by Covid-19 versus other types of deaths (Eisma et al, 2021).
Most participants were supported by friends and family, but 39% reported difficulties
getting this support. A quarter reported that their friends or family were
unable to support them in the way that they wanted, with a fifth feeling
uncomfortable asking for help. People described how they missed being able to
hug their friends and family, and the difficulties they experienced talking
openly about their feelings, especially over the phone or internet.
A general lack of understanding and empathy within social networks was commonly
perceived. Due to the widespread stress caused by the pandemic, people worried
about adding to the emotional and mental health burden of friends and family,
who had their own issues to deal with. People also felt that (non-bereaved)
others could not understand what they were going through due to the exceptional
nature of pandemic bereavement (Harrop et al, 2021a).
Bereaved
people also commonly described problems relating to workplaces. These included
perceived insensitivity and a lack of understanding and compassion among
managers and colleagues. At a time of financial uncertainty, people were
disinclined to take leave from work out of fear of losing their jobs or livelihoods.
People in frontline jobs described difficulties managing their grief and
working in pressured, public-facing roles, while others described the isolating
effects of being furloughed or working remotely, which made it harder for them
to connect with and feel supported by their colleagues (Torrens-Burton et al,
2021).
For
families living together, lack of time and space during lockdowns, and periods
of school closure, made it harder for them to process and find respite from
their grief (Torrens-Burton et al, 2021). Although most parents felt that their
children were coping well with family-based support, some reported that their
children found it difficult to open up to them. Parents and guardians also
described the challenges of supporting their children while also struggling
with their own grief and trying to protect them (Harrop
et al, 2021b), a problem similarly observed among bereaved relatives in another
UK study (Rapa et al, 2021).
Participants
with children described the added strain caused to their children by school and
university closures, and associated disruption to their child's daily routines
and relationships. However, parents also positively described support received
through schools. Some children were receiving specialist emotional support,
which although helpful stopped during periods of school closure. Other parents
described the more general support provided by schools and teachers. Valued
features of this support included checking in on students during closure
periods, being aware of the student's bereavement circumstances and potential
problems, having informal conversations with students and their parents about
their grief, and proactively offering or placing students on the 'radar' for
specialist emotional support if needed (Harrop et al,
2021b).
Access to bereavement and mental
health services
We found
that just over half of our participants experienced high emotional support
needs and vulnerability in grief. However, three quarters of these more
vulnerable participants were not accessing bereavement counselling
or mental health support (Harrop et al, 2021a).
So what
explains this low uptake of formal support? Only 29% of people felt that they
did not need bereavement service support due to sufficient support from friends
and family (Harrop et al, 2021a), however 60% of
people had not tried to access bereavement services. Of those
who had sought support, over half experienced difficulties accessing these
services. People reported a lack of appropriate support, feeling
uncomfortable asking for support and being unsure if it would help them. Some
felt unhappy discussing their grief over the phone or video-call. There was
also a perceived need for Covid-19-specific bereavement support as well as for
culturally relevant and group-specific support for those with shared
experiences. People who lost elderly parents to long-term illnesses (and in
some cases Covid-19) felt less entitled due to the perceived greater needs of
others and the heavy demand being placed on services as a result of the
pandemic. People also reported not knowing how to access bereavement service
support (Harrop et al, 2021a). Relatedly, we found
that only a third of bereaved people had been given information about
bereavement support services, with those bereaved in non-hospice settings less
likely to be given this information, suggesting a missed opportunity for
provision of such information, especially in hospital and care-home settings
(Selman et al, 2021a).
Around a
quarter of parents described needing additional support from bereavement or
mental health services for their children, but in just over a third of cases
were not receiving this support. Reasons why some children and young people
were not getting the support they needed included unavailability of, or delayed
referrals to, mental health services due to the pandemic, long waiting times
for support, not knowing how to get support, preferences for face-to-face
support, and resistance from their children to receiving external support (Harrop et al, 2021b). Rapa et al (2021) report that only a
tenth of relatives bereaved during the pandemic were asked about their deceased
relative's relationships with children, further suggesting that important
opportunities for providing families with information about child grief and
support services may have been missed.
Conclusions
This synthesis
of results from the Bereaved during
COVID-19 study demonstrates the exceptional challenges of pandemic
bereavement, including high levels of disruption to end-of-life, death and
mourning practices as well as to people's social networks and usual coping
mechanisms. We identified considerable needs for emotional and therapeutic
support among bereaved people alongside significant difficulties in receiving
and accessing support, including for their children. Across our five
publications, we have made the following recommendations for improving the
experiences of adults, children and young people bereaved during and following
this and future pandemics.
1
Reducing
the trauma associated with death experiences, through improved communication
with and involvement of families (Selman et al, 2021a), safe facilitation of
family visiting to healthcare settings, and, where this is not possible,
connecting families and loved ones through accessible remote communication
methods (Torrens-Burton et al, 2021).
2
Improving
family support immediately after a death, including routinely providing
opportunities to discuss patient care and the circumstances of the death, and
information about locally and nationally available bereavement support for
adults, children and young people (Torrens-Burton et al, 2021).
3
Greater
resourcing and expansion of national and regional adult and child bereavement
services, including culturally-competent support, tailored to the needs of
those bereaved during the Covid-19 pandemic, and specific support for groups
with shared experiences and characteristics.
4
Implementing
strategies to improve awareness of bereavement support options for adults and
children and young people, including information on services, self-help
resources and materials for different age groups, promoted and made available
online and in community settings (Harrop et al,
2021a, 2021b).
5
Mitigating
loneliness and social isolation, including flexible support bubble arrangements
for the recently bereaved when restrictions are in place and informal
community-based interventions aimed at strengthening social networks, grief
literacy and communication skills, with regards to children and adults (Harrop et al, 2021a, 2021b).
6
Training
for school staff to have age-appropriate conversations with students around
grief and bereavement, and to be able to identify when a child might need
additional specialist support. During lockdown periods of school closure
specialist programmes should continue for existing
students (remotely if needed), while also proactively identifying and engaging
with newly bereaved families who may need support (Harrop
et al, 2021b).
7
Developing,
promoting and adhering to guidance and best practice recommendations regarding:
a) funeral options during times of social restrictions, b) supporting those
administering the death of their deceased relative, and c) supporting bereaved
employees (Torrens-Burton et al, 2021).
8
Providing
opportunities for remembrance, greater respect and listening to those bereaved.
This means recognising the potentially dehumanising and alienating consequences of death
statistics and conspiracy theories in mainstream and social media; facilitating
national and local initiatives which support private and public remembrance;
and inclusive consultation with those recently bereaved (eg
via the UK Commission on Bereavement: bereavementcommission.org.uk) to improve
support for bereaved people and ensure lessons are learned for future
pandemics. (Torrens-Burton et al, 2021).
References
Becque
YN, van der Geugten W, van der Heide
A, Korfage IJ, Pasman HRW, Onwuteaka‐Philipsen BD et al (2021) Dignity
reflections based on experiences of end‐of‐life care during the first wave of the COVID‐19 pandemic: A qualitative inquiry among bereaved relatives in the Netherlands
(the CO‐LIVE study). Scandinavian
Journal of Caring Sciences. https://doi.org/10.1111/scs.13038
Breen LJ,
Mancini VO, Lee SA, Pappalardo EA, Neimeyer RA (2021) Risk factors for dysfunctional grief and
functional impairment for all causes of death during the COVID-19 pandemic: The
mediating role of meaning. Death Studies. https://doi.org/10.1080/07481187.2021.1974666
Eisma MC,
Tamminga A, Smid GE & Boelen PA (2021) Acute grief after deaths due to COVID-19,
natural causes and unnatural causes: An empirical comparison. Journal of
Affective Disorders, 278, 54–56.
https://doi.org/10.1016/j.jad.2020.09.049
Harrop E,
Farnell D, Longo M, Goss S, Sutton E, Seddon K et al (2020) Supporting people bereaved during
COVID-19: Study Report 1, 27 November 2020. Cardiff
University and the University of Bristol. Available at:
www.covidbereavement.com (accessed 4 December 2021).
Harrop
EJ, Goss S, Farnell DJ, Longo M, Byrne A, Barawi K et al (2021a) Support needs and barriers to
accessing support: Baseline results of a mixed-methods national survey of
people bereaved during the COVID-19 pandemic. Palliative Medicine.
https://doi.org/10.1177/02692163211043372
Harrop E,
Goss S, Longo M, Seddon K, Torrens-Burton A, Sutton E
et al (2021)b Parental perspectives on the grief and
support needs of children and young people bereaved during the Covid-19
pandemic: qualitative findings from a national survey. medRxiv 2021.12.06.21267238.
https://doi.org/10.1101/2021.12.06.21267238
Hanna JR,
Rapa E, Dalton LJ, Hughes R, McGlinchey T, Bennett KM
et al (2021) A qualitative study of bereaved relatives'
end of life experiences during the COVID-19 pandemic. Palliative
Medicine, 35(5) 843–51. https://doi.org/10.1177/02692163211004210
Mayland
CR, Hughes R, Lane S, McGlinchey T, Donnellan W, Bennett K et al (2021) Are public health
measures and individualised care compatible in the
face of a pandemic? A national observational study of
bereaved relatives' experiences during the COVID-19 pandemic. Palliative
Medicine. https://doi.org/10.1177/02692163211019885
Menzies RE, Neimeyer
RA, Menzies RG (2020) Death anxiety, loss, and grief
in the time of COVID-19. Behaviour Change, 37(3)111–5.
https://doi.org/10.1017/bec.2020.10
Neimeyer
RA, Lee SA (2021) Circumstances of the death and associated risk factors for
severity and impairment of COVID-19 grief. Death Studies, May 21, 1–9.
https://doi.org/10.1080/07481187.2021.1896459
Rapa E,
Hanna JR, Mayland CR, Mason S, Moltrecht
B & Dalton LJ (2021) Experiences of preparing children for a death of an
important adult during the COVID-19 pandemic: a mixed methods study. BMJ open.
Aug 1, 11(8):e053099.
https://doi.org/10.1136/bmjopen-2021-053099.
Selman LE, Farnell DJ, Longo M, Goss S, Seddon
K, Torrens-Burton A et al (2021a) Place, cause and expectedness of death and
relationship to the deceased are associated with poorer experiences of
end-of-life care and challenges in early bereavement: Risk factors from an
online survey of people bereaved during the COVID-19 pandemic. medRxiv.
https://doi.org/10.1101/2021.09.09.21263341
Selman E, Sowden R & Borgstrom E
(2021b) 'Saying goodbye' during the COVID-19 pandemic: A document analysis of
online newspapers with implications for end of life care. Palliative Medicine.
https://doi.org/10.1177/02692163211017023.
Selman LE,
Chamberlain C, Sowden R, Chao D, Selman D, Taubert M et al (2021c). Sadness, despair and anger when a
patient dies alone from COVID-19: A thematic content analysis of Twitter data
from bereaved family members and friends. Palliative
Medicine, 35(7) 12671276. https://doi.org/10.1177/02692163211017026
Sue Ryder
(2020) Bereaved people claim lockdown deaths became just a statistic. Available
at: www.sueryder.org/news/bereaved-people-claim-lockdown-deaths-became-just-a-statistic
(accessed 4 December 2021).
Sowden R,
Borgstrom E, Selman LE
(2021) 'It's like being in a war with an invisible enemy': A document analysis
of bereavement due to COVID-19 in UK newspapers. PLoS
one. 16(3):e0247904.
Torrens-Burton
A, Goss S, Sutton E, Barawi K, Longo M, Seddon K (2021) 'It was brutal. It still is': A qualitative
analysis of the challenges of bereavement during the COVID-19 pandemic reported
in two national surveys. medRxiv
2021.12.06.21267354. https://doi.org/10.1101/2021.12.06.21267354
Acknowledgements
Our thanks
to everyone who completed the survey for sharing their experiences, and to all
the individuals and organisations that helped
disseminate the survey. We would also like to thank our research team and
advisory group members for their contributions to the study.
Funding
The Bereavement during COVID-19 study is funded by the UKRI/ESRC (Grant No. ES/V012053/1). Emily Harrop's post is supported by Marie Curie core grant funding to the Marie Curie Palliative Care Research Centre, Cardiff University (grant MCCC-FCO-11-C).